Multidisciplinary Team (MDT) Approach to Diagnosis & Management of Perianal Crohn's Disease
David P. Hudesman, MD
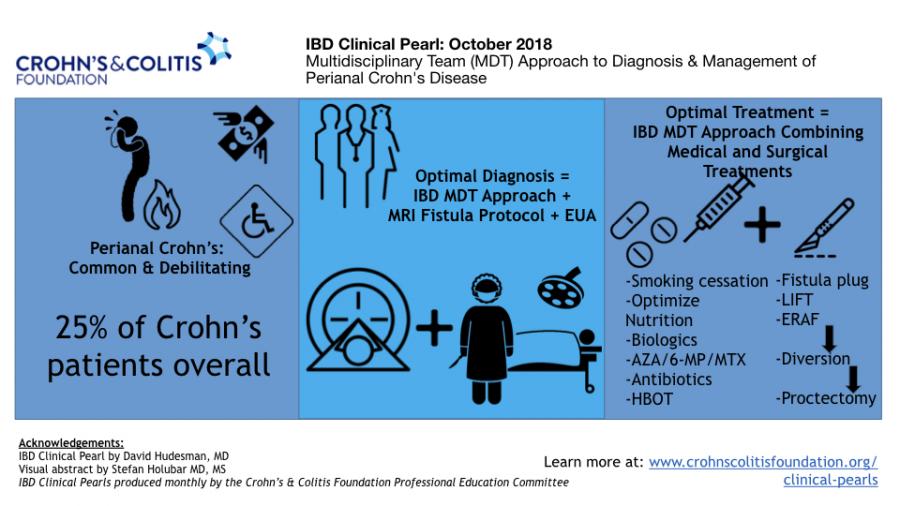
Perianal Crohn’s disease (CD) is often a debilitating condition, negatively impacting patient quality of life. Approximately 26% of Crohn’s patients will develop a perianal fistula, and in about 5% of patients a perianal fistula will be the only manifestation. Patients with perianal CD are more likely to have a complicated disease course with increased rates of extra intestinal manifestations, perianal abscesses, deep anal canal ulcers, luminal fistulas and strictures, surgeries and steroid resistance. Diagnosis and management of perianal Crohn’s requires an expert, multidisciplinary approach.
Optimal diagnosis and evaluation of perianal CD combines an imaging modality, ideally pelvic magnetic resonance imaging (MRI) fistula protocol, with an exam under anesthesia (EUA) performed by a colorectal surgeon. MRI is the most common imaging modality that is used, but in experienced hands endoscopic ultrasound (EUS) may be done as well. When combining a MRI or EUS with an EUA, diagnostic accuracy is close to 100%.
Co-management with a surgeon and a gastroenterologist is crucial with perianal CD. Drainage of an abscess and possible seton placement to prevent future septic complications is the critical first step. TNF inhibitors (TNFi) have the best evidence for decreasing perianal drainage and fistula healing. In the ACCENT II trial, Infliximab treated patients had a fistula closure rate of 36% at one year. Subgroup analyses have shown fistula healing with adalimumab and certolizumab as well. In addition, small observational studies have shown potential benefit of Vedolizumab and Ustekinumab in perianal CD. In a recent multicenter retrospective cohort study on 253 patients, multimodal therapy, which includes aTNFi +/- an immunomodulator and antibiotics, along with EUA and draining seton placement, led to a 52% complete fistula healing rate. Of note antibiotics can decrease drainage and improve QoL but do not aid healing and should not be used for un-drained perianal abscesses. Patients must understand the importance of smoking cessation.
Refractory fistulas require further surgical interventions. Sphincter-preserving approaches are 1st line including subcutaneous fistulotomy, fistula plug insertion, Ligation of the Intersphincteric Tract (LIFT) procedure, or endorectal advancement flap (ERAF) usually in combination with TNFi and immunomodulation ala SONIC trial. More aggressive options include fecal diversion with a loop ileostomy (only 17% of patients can be reversed successfully), and proctectomy; however proctectomy in this setting is associated with difficulities with wound healing resulting in persistent perineal sinus. Two emerging treatments include hyperbaric oxygen therapy (HBOT) and mesenchymal stem cells (MSC). A recent small case series study showed HBOT resulted in healing in 65% of perianal fistulae. In a phase III study of allogenic adiposed-derived MSCs, 50% of treated patients had fistula healing compared to 34% of placebo. Larger multicenter phase III trials are currently underway.
References:
- Schwartz DA, Loftus EV, Tremaine WH et al. The natural history of fistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology 2002;122(4):875-880.
- Schwartz DA, Wiersema MJ, Dudiak KM, et al. A comparison of endoscopic ultrasound, magnetic resonance imaging, and exam under anesthesia for evaluation of Crohn’s perianal fistulas. Gastroenterology 2001;121(5):1064-1072.
- Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. New England Journal of Medicine 2004;350(9):876-885.
- Sebastian S, Black C, Pugliese D et al., The role of multimodal treatment in Crohn’s disease patients with perianal fistula: a multicentre retrospective cohort study. Alimentary Pharmacology and Therapeutics 2018: 1-10.
- Panes J, Garcia-Omo D, Van Assche G, et al. Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn’s disease: a phase 3 randomized, double-blind controlled trial. Lancet 2016;108(10):1666-1668.