Colorectal Cancer Risk in IBD
Colorectal cancer risk and IBD
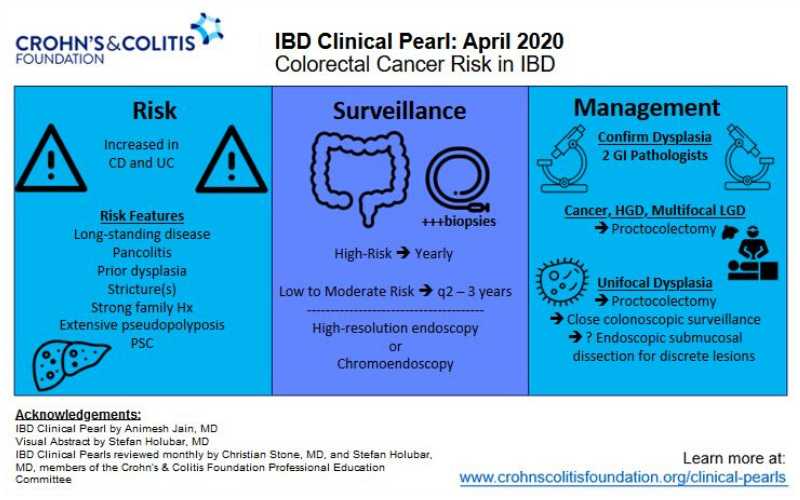
Patients with IBD appear to be at notably increased risk of colorectal cancer compared to the general population [1-3], with one recent study demonstrating a 7% colorectal cancer risk after 30 years of disease [4]. Patients with at least 8 years disease duration and colonic involvement are at increased risk of colorectal cancer (excluding patients with only ulcerative proctitis, or with Crohn’s disease and less than 1/3 of the colon involved). Patients at risk of colorectal cancer should be enrolled in a dysplasia surveillance plan as this appears to reduce the risk of colorectal cancer[5]. Surveillance typically includes colonoscopy every 1-3 years, depending on individual patient risk [6, 7].
Risk factors and surveillance intervals
In patients at high risk, consider ~1 year surveillance intervals. High risk features include: primary sclerosing cholangitis (PSC), prior history of dysplasia or colonic strictures, or strong family hx of colorectal cancer (e.g., 1st degree relative with CRC < age 50). Patients with low to moderate risk may be surveyed every 2-3 years. Moderate risk features include: extensive colitis with moderate inflammatory burden, family hx of CRC in first degree relative > age 50 and possibly extensive inflammatory polyps or pseudopolyps [6, 8]
Surveillance Protocols
Most colonic dysplasia should be visible, hence a thorough high-quality exam is essential. High definition colonoscopes are preferred. Use of dye spray (chromoendoscopy) may have additional benefits for detecting dysplasia[9-13]. Random biopsies are typically performed in 4 quadrant fashion every 10cm. However, yield from random biopsies is low and this could be skipped if chromoendoscopy is utilized[8].
Management of Endoscopic lesions
Any visible polyps or lesions should be endoscopically resected if feasible and the specimen should be sent in a separately labeled jar. If a lesion has indistinct borders or is not amenable to resection, biopsy sample should be taken and sent in a separate jar[6, 8].
Management of Dysplasia
A diagnosis of dysplasia should ideally be confirmed by two experienced pathologists. Dysplasia should be managed closely and aggressively to prevent progression to cancer. For any confirmed case of high-grade dysplasia or multi-focal low-grade dysplasia, proctocolectomy should be recommended. For isolated unifocal dysplasia, options include proctocolectomy or close colonoscopic surveillance.