Fistulizing Crohn's Disease
What is Fistulizing Crohn’s Disease?
Fistulizing Crohn’s disease may present in patients with Crohn’s disease over their lifetime1,2 and can occur anywhere along the GI tract, affecting portions such as the small intestine, colon, rectum, or the anus.3,4
It is common for people with fistulas to feel stress, anxiety, and other mental and emotional concerns about body image and intimacy.5 If you are experiencing these concerns, speak with your healthcare team to discuss options for connecting with a mental health professional who can provide helpful coping strategies. The Foundation’s support programs can also offer connection to others who may have similar experiences.
Types and Symptoms of Fistulas
A fistula is an abnormal connection or tunneling between the intestines and a nearby organ or skin. Fistulas form when inflammation causes sores or ulcers on the inside wall of the intestine or nearby organs. Those ulcers can extend through the entire thickness of the bowel wall, creating a tunnel to drain the pus from the infected area. An abscess, or a collection of pus, can also cause a fistula to form.
Below are different types of fistulas found in Crohn’s disease. (Please note: Medications aim to treat the underlying active disease; surgical procedures may be considered but not every fistula requires treatment.)
| Type of Fistula | Description | Possible Symptoms |
|---|---|---|
| Perianal Fistula | A tunnel/connection between the anal canal and/or rectum and the surface of skin in the anal area | Tender swelling or lump in area around the anus; pain and irritation when sitting, moving, having a bowel movement, or coughing; drainage/discharge; and/or bleeding |
| Rectovaginal or colovaginal fistulas | A tunnel/connection between the intestines and the vagina | Passing air, stool, or pus through the vagina; brown/foul-smelling discharge; and/or painful intercourse |
| Enteroenteric fistulas | A tunnel/connection from one part of the intestines to another part of the intestines | Diarrhea (can feel like a flare), poor absorption of nutrients, and/or dehydration, and/or no symptoms at all |
| Enterocutaneous or colocutaneous fistulas | A tunnel/connection from the intestines to the surface on the skin | Leaking of stool, which may include a foul smell, brown discharge, redness, and/or pain |
| Enterovesical or colovesical fistulas | A tunnel/connection from the intestines to the bladder | Passing air, stool, or pus when urinating; foul-smelling urine, urine leaking from anus, frequent urination, and/or frequent urinary tract infections (UTIs) |
| Enterocolonic fistulas | A tunnel/connection from the colon to another part of the intestines | Diarrhea (can feel like a flare), poor absorption of nutrients, dehydration, and/or no symptoms at all |
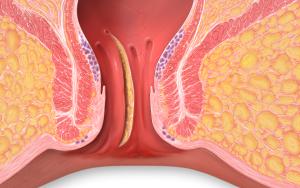
- Perianal Fistulas

Perianal fistulas are abnormal tracts or “tunnels” between the anal canal or rectum and an external opening in the skin near the anus and are the most common type of fistula in Crohn’s disease. This can be referred to as perianal Crohn’s disease or perianal fistulizing disease. These fistulas can be painful, especially if there is an abscess or infection at the site. They can cause leakage of stool, pus, or blood that you may see on your underwear.
Diagnosis of Perianal Crohn’s Disease
Perianal fistulas are often diagnosed by previous medical history and a physical examination looking at the skin around the anal area. Your physician may suggest additional testing, such as an MRI of the pelvis, endoscopic ultrasound, or an examination under anesthesia, to help determine the extent of disease.6
Treatments for Perianal Crohn’s Disease
A combination of medical and surgical treatments (oftentimes more than one surgical procedure) is the best approach to treat perianal Crohn’s disease.
Medications
IBD medications aim to treat underlying disease and infection, which are often the best way to avoid complications, like fistulas. However, there may be times when a fistula might develop, and you may need additional medications to treat the fistula and help with the discomfort.
Antibiotics, such as metronidazole and ciprofloxacin, are an important part of the treatment of a perianal fistula. They can help clear up infections and may decrease drainage. However, antibiotics are not a long-term therapy and should be used in the short term to treat any infection along with long-term maintenance medications.
Biologic anti-TNF medications have been shown to be effective in reducing drainage and promoting healing. Thiopurines, such as azathioprine and 6-MP, are commonly prescribed in combination with anti-TNF medications to improve overall response, decrease antibody formation, and achieve remission. Additionally, newer biologics, such as vedolizumab, ustekinumab, and risankizumab, have also been shown to be effective in the treatment of Crohn’s perianal fistulas. Your doctor will work with you to create a treatment plan, and it may include biologic medications, or a combination of other treatments. Talk to your doctor to understand your options.
Please note: Corticosteroids should be avoided when experiencing a perianal fistula as they have been shown to lead to more abscesses and worsening fistulas.
Procedures and Surgery
Having surgery can be beneficial in helping a fistula heal and may depend on where your fistula is located. The goal of surgery is to heal the perianal fistula while avoiding damage to anal sphincter muscles as these muscles surround the area and control the elimination of stool. If there is an abscess, a colorectal surgeon trained in management of Crohn’s abscesses and fistulas will surgically drain the abscess.
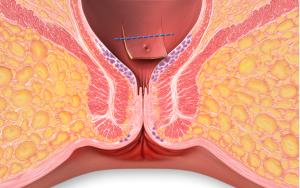
Setons

Seton
Seton placement is one option to help heal perianal fistulas. A seton is a thin rubber surgical thread that is placed through the fistula tract and exits out through the anus. The seton is then tied to form a loop, with the end of the loop hanging out of the anus. This allows the tract to stay open for the fistula to drain which helps avoid infectious complications. The seton is left in for at least several months and then potentially removed once the fistula has drained in some instances. The seton can be removed in the office or in the operating room if it requires additional surgery. After the infection is cleared, medical management to control the inflammation is required to continue healing the fistula tract.
Surgery
Once a combination of seton placement and medical management has controlled the infection and inflammation, surgical procedures may be considered by a colorectal surgeon when a patient is in remission. Such procedures include:

Fistulotomy
Fistulotomy: This is a surgical procedure to divide the fistula tract. The primary goal is to repair the fistula without damaging the anal sphincter muscles, which help you hold fecal material in your rectum. In this procedure, the length of the fistula is cut open and flattened out, obliterating the communication between the skin and the rectum or anus. This procedure is suitable for simple fistulas that either don’t cross the sphincter muscle at all or only pass through a small amount of muscle.
Advancement Flap
Advancement Flaps: After the fistula tract has been cleaned, the inside lining of the rectum is lifted and pulled down inside the anal canal to cover the internal opening of the fistula. This procedure is used for complex fistulas where sphincter muscles are involved and have not been controlled/healed with medical therapy.
LIFT Procedure
LIFT Procedure: Ligation of intersphincteric fistula tract (LIFT) procedures are performed by colorectal surgeons for complex fistulas. The surgeons make a small cut just outside the entrance of the anal canal to reach the space between the internal and external anal sphincter muscles. Once the fistula tunnel is located, it is cut in two, and then both ends are stitched and closed.
There are many new therapies and options becoming available with great promise. Stem cell therapy is an emerging area with promising results in healing perianal fistula. This option is not yet approved in the United States but is approved in several European countries. Clinical trials are concluding in the U.S. with anticipation for approval in the next several years. Additionally, multiple other stem cell products are being studied to continue to improve outcomes.
- Rectovaginal Fistulas
A rectovaginal fistula is a connection between the rectum or anus and the vagina. This connection allows gas or stool to leak through the fistula and pass into the vagina. Symptoms may include painful intercourse, perianal pain, and vaginal irritation. Medications aim to treat the underlying active disease, though surgical procedures may still be considered. Such procedures include flap and LIFT procedure, folding a flap of healthy tissue over the fistula opening, which is known as a vaginal advancement flap, or using the skin of the vaginal lip to close the fistula. Consider having an open discussion with your provider about the best treatment options for your individual case.
- References
- Scharl M, Rogler G, Biedermann L. Fistulizing Crohn’s Disease. Clin Transl Gastroenterol. 2017;8(7):e106. Published 2017 Jul 13. doi:10.1038/ctg.2017.33.
- Gastroenterology. 2000;119:1132-1147.
- Cosnes J et al. Long-term evolution of disease behavior of Crohn’s disease. Inflamm Bowel Dis. 2002;8:244–250.
- Gower-Rousseau C et al. Epidemiology of inflammatory bowel diseases: new insights from a French population-based registry (EPIMAD). Dig Liver Dis. 2013;45:89–94.
- Adegbola SO, Dibley L, Sahnan K, et al. Burden of disease and adaptation to life in patients with Crohn’s perianal fistula: a qualitative exploration. Health Qual Life Outcomes. 2020 Nov 20;18(1):370.
- Schwartz DA, Wiersema MJ, Dudiak KM, et al. A comparison of endoscopic ultrasound, magnetic resonance imaging, and exam under anesthesia for evaluation of Crohn’s perianal fistulas. Gastroenterology. 2001;121(5):1064–1072.
This program is generously supported, in part by, Takeda Pharmaceuticals
Related Resources
Brochure
Surgery for Crohn's Disease and Ulcerative Colitis...